



By Mindnesto Editorial Team · Updated June 2026 · 11 min read
Reviewed for medical accuracy — sources cited from NHS, NICE, APA, NIMH and peer-reviewed clinical psychology research
Panic attacks are one of the most terrifying experiences the human nervous system can produce — and one of the most misunderstood. If you have experienced a attack, you already know that describing the experience to someone who has not had one is almost impossible. Your heart hammers. Your chest tightens. The world suddenly feels unreal. And somewhere behind all of it, a voice insists that this time — this one — is genuinely the end.
Yet panic attacks are neither random nor mysterious. The cause behind panic attacks are among the most extensively researched topics in clinical psychology — and understanding the science behind why panic attacks happen is genuinely, clinically therapeutic. Research published in Behaviour Research and Therapy demonstrates that psychoeducation about panic attacks — simply learning what they are, why they happen, and what maintains them — produces measurable reductions in panic attack frequency and severity even before any other treatment is applied.
This guide covers the complete science of panic attacks — from the neurobiology of what happens in your brain during an attack, to the psychological maintaining mechanisms that turn occasional panic into panic disorder, to the most evidence-based 2026 approaches to treatment and recovery.
We have connected this to our practical guide on how to stop a panic attack in 5 minutes and our broader anxiety guide — because understanding panic attacks in depth complements the practical intervention tools covered in those posts.
⚠️ Medical Disclaimer: This article is for informational and educational purposes only. Panic attacks can occasionally resemble symptoms of medical conditions including cardiac events. If you experience chest pain, breathlessness, or any physical symptoms for the first time — always seek medical assessment before assuming panic. If you are in crisis, please contact emergency services or a crisis line immediately.
What Are Panic Attacks — The Clinical Definition
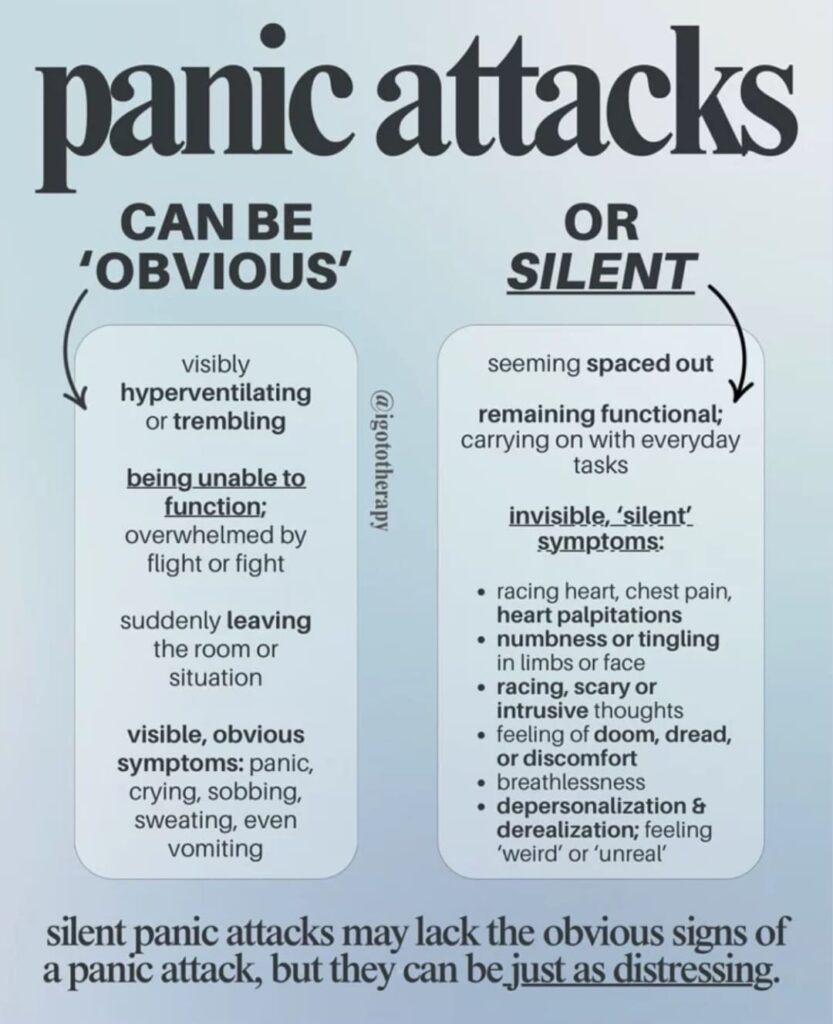
They are defined by the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition) as discrete episodes of intense fear or discomfort that reach peak intensity within 10 minutes and are accompanied by at least four of the following physical and psychological symptoms:
- Racing or pounding heartbeat (palpitations)
- Sweating — often sudden and profuse
- Trembling or shaking
- Shortness of breath or feeling of smothering
- Choking sensation
- Chest pain or chest tightness
- Nausea or abdominal distress
- Dizziness, lightheadedness, or feeling faint
- Chills or hot flushes
- Tingling or numbness sensations (paraesthesia)
- Derealisation — feelings that surroundings are unreal
- Depersonalisation — feeling detached from yourself
- Fear of losing control or “going crazy”
- Fear of dying
Attacks are classified as unexpected (occurring with no obvious trigger), situationally bound (reliably occurring in specific situations), or situationally predisposed (more likely but not inevitable in specific situations). This distinction matters clinically because it shapes both the psychological maintaining mechanisms and the most effective treatment approach.
Panic Attacks vs Panic Disorder — A Critical Distinction
Single attacks are extremely common — research suggests that approximately 35% of adults experience at least one attack in their lifetime. However, attacks become panic disorder only when they are followed by persistent concern about future attacks, significant changes in behaviour to avoid triggers, or functional impairment lasting at least one month.
According to the National Institute of Mental Health (NIMH), panic disorder affects approximately 2.7% of US adults in any given year — with significantly higher rates in women than men, and peak onset typically in late adolescence and early adulthood.
The NHS estimates that panic disorder affects approximately 1 in 100 people in the UK, with many more experiencing recurrent panic attacks that do not meet full diagnostic criteria but nonetheless significantly impair quality of life.
The Neuroscience — What Happens in Your Brain
To truly understand attacks, you need to understand what is happening in your brain and body during an episode. This knowledge is itself therapeutic — because panic attacks derive much of their power from their apparent mystery and unpredictability.
The Amygdala — Your Brain’s Panic Button
The attack begins in the amygdala — the almond-shaped structure deep in your brain’s temporal lobe that serves as its primary threat-detection and alarm system. The amygdala continuously monitors incoming sensory information — what you see, hear, smell, feel, and crucially what you sense from inside your own body — and compares it against a threat library built from past experience.
When the amygdala detects what it interprets as a threat — real, remembered, or imagined — it fires an emergency signal that bypasses the rational prefrontal cortex entirely. This is intentional: in a genuine life-threatening situation, you do not want to think carefully before responding. You need to react immediately.
The amygdala’s alarm signal reaches the hypothalamus within milliseconds, triggering the activation of the sympathetic nervous system — the biological system responsible for the fight-or-flight response.
The Fight-or-Flight Response — The Biology of Attacks
The sympathetic nervous system activation that characterises panic attacks produces a cascade of rapid physiological changes designed — in genuinely dangerous situations — to maximise survival:
Adrenaline (epinephrine) and norepinephrine flood the bloodstream from the adrenal glands. These stress hormones produce the following panic attack symptoms within seconds:
- Heart rate increases dramatically — pumping oxygenated blood to muscles preparing for fight or flight. This produces the palpitations and chest tightness characteristic of panic attacks.
- Breathing rate increases and shallows — to take in more oxygen. This produces the breathlessness and hyperventilation of panic attacks.
- Blood vessels constrict at the periphery and dilate at core muscles — producing the tingling, numbness, and cold sensations in hands and feet during panic attacks.
- Blood is redirected away from the digestive system — producing the nausea and abdominal discomfort of panic attacks.
- Pupils dilate and perception narrows — producing the tunnel vision and sense of unreality (derealisation) during panic attacks.
- Sweating increases — as the body’s cooling system activates in anticipation of physical exertion.
Every single physical symptom of attack is therefore a direct consequence of a biological system doing precisely what it evolved to do. The problem is not that the system is broken — it is that it has been activated in the absence of a genuine physical threat.
The Carbon Dioxide Sensitivity Theory of Panic Attacks
One of the most important and least widely understood neuroscientific findings about panic attacks involves carbon dioxide (CO₂) sensitivity. Research by Dr. Donald Klein of the New York State Psychiatric Institute found that people with panic disorder show a significantly heightened sensitivity to elevated CO₂ levels — which normally serve as the brain’s signal that breathing is insufficient.
In people prone to attacks, even mild elevations in CO₂ — produced by slight hyperventilation or breath-holding — trigger an alarm response disproportionate to the actual physiological need. This CO₂ hypersensitivity explains several important panic attack phenomena:
- Why hyperventilation both produces and worsens attack symptoms
- Why slow, diaphragmatic breathing is so immediately effective during attacks — it directly addresses CO₂ imbalance
- Why panic attacks frequently occur at night when CO₂ naturally rises slightly — explaining nocturnal panic attacks
- Why physical exertion can trigger attacks in susceptible individuals — exercise raises CO₂
This CO₂ sensitivity theory has significant implications for understanding attacks as having a genuine physiological substrate — not simply a psychological one.
The Psychology Behind Attacks — The Cognitive Models
The neuroscience explains what happens physically during attacks. The psychology explains why panic attacks develop, why they recur, and why some people develop panic disorder while others experience isolated episodes.
Clark’s Cognitive Model of Panic Disorder — 1986 to 2026
The most influential psychological model of panic attacks is Dr. David Clark’s Cognitive Model of Panic, first published in Behaviour Research and Therapy in 1986 and still regarded as the foundational theoretical framework for understanding and treating panic disorder.
Clark’s model proposes that panic attacks are maintained by a specific cognitive pattern: the catastrophic misinterpretation of benign bodily sensations.
The cycle works as follows:
- A triggering stimulus — either external (a stressful situation) or internal (a physical sensation such as a slightly elevated heart rate, dizziness, or breathlessness) — is noticed
- The individual catastrophically misinterprets this sensation as evidence of imminent danger — “My heart is racing — I am having a heart attack” or “I feel dizzy — I am going to faint/die”
- This catastrophic interpretation triggers anxiety and fear
- Anxiety activates the fight-or-flight response — which produces exactly the physical sensations being catastrophically misinterpreted
- The intensified physical sensations appear to confirm the catastrophic interpretation — creating a self-amplifying feedback loop that reaches peak intensity within minutes
- The loop is a panic attack
The elegance — and clinical importance — of Clark’s model lies in what it reveals about the maintaining mechanism: it is not the original physical sensation that causes the attack. It is the meaning applied to that sensation. Consequently, changing the meaning — learning to interpret elevated heart rate or dizziness as normal anxiety symptoms rather than signs of imminent death — is the core mechanism through which CBT breaks the terror attack cycle.
Barlow’s False Alarm Theory — Why Crisis Attacks Feel So Real
Dr. David Barlow of Boston University proposed a complementary model — the False Alarm Theory — that explains the initial occurrence of stress attacks and the development of panic disorder.
Barlow proposed that a crisis attack begins with a true alarm — the fight-or-flight response activated by a genuinely stressful event. However, through a process of learning and conditioning, the physiological response becomes associated with the context in which it occurred — even when that context is not genuinely dangerous. Subsequent exposure to similar contexts (or even to internal sensations resembling those of the original alarm) can trigger a false alarm — a full fight-or-flight response in the absence of genuine threat.
Over time, if the individual begins to fear the alarm itself — developing what Barlow termed anxiety sensitivity — the stage is set for stress disorder. Anxiety sensitivity — the belief that anxiety sensations are themselves dangerous — is the most reliable psychological predictor of panic disorder development, more predictive even than trait anxiety.
Interoceptive Conditioning — Why Attacks Seem Unpredictable
Dr. Ronald Rapee of Macquarie University contributed the concept of interoceptive conditioning to the psychology of terror attacks — explaining why attacks often appear to occur “out of nowhere.”
Interoceptive conditioning describes the process through which internal bodily sensations — the beating of the heart, a change in breathing rate, slight dizziness, physical warmth — become conditioned stimuli for stress attacks, even in the complete absence of external threat.
After several attacks, the individual’s amygdala learns to associate certain physiological states with the catastrophic experience of stess. Consequently, even slight changes in those physiological states — produced by exercise, caffeine, sexual arousal, or simply becoming warm — can trigger a conditioned alarm response that escalates into a full dread attack. This explains why stress attacks appear to occur spontaneously and unpredictably — when in reality they are being triggered by misinterpreted internal signals that the individual has not learned to recognise.
What Maintains Attacks — The Vicious Cycles
Understanding what turns isolated panic attacks into panic disorder requires understanding the maintaining mechanisms — the patterns of thought and behaviour that keep the cycle running.
Safety Behaviours — The Maintaining Mechanism Nobody Talks About
Safety behaviours are the specific actions people take during or after attacks to prevent the feared catastrophe. Common examples include:
- Sitting down immediately when feeling dizzy — to prevent fainting
- Gripping a fixed object during attacks — to counteract feeling of unreality
- Keeping a phone in hand at all times — to be able to call for help
- Avoiding exercise — in case elevated heart rate triggers attacks
- Carrying medication in case of — even without taking it
- Leaving situations quickly when attacks begin
Safety behaviours are maintained because they appear to work — the feared catastrophe does not occur. However, they maintain stess disorder by preventing the individual from discovering that the catastrophe would not have occurred anyway. Consequently, safety behaviours are one of the primary targets of CBT for panic disorder — their gradual elimination is essential for recovery.
Anticipatory Anxiety and Avoidance
Following attacks, many people develop anticipatory anxiety — persistent worry about when the next panic attack will occur — and begin systematically avoiding situations, places, or activities associated with previous attacks.
This avoidance initially reduces distress. Over time, however, it narrows life significantly, reinforces the message that avoided situations are genuinely dangerous, and maintains the amygdala’s threat associations. Furthermore, avoidance behaviour can develop into agoraphobia — avoidance of situations from which escape might be difficult during attacks — in a significant minority of people with stress disorder.
Research published in Journal of Anxiety Disorders found that avoidance behaviour was the single strongest predictor of terror disorder severity and chronicity — confirming that what you avoid continues to frighten you.
2026 Advances in Understanding and Treating
Interoception Training — A 2026 Frontier in Panic Treatment
One of the most exciting developments in stress attack science in 2026 is the growing body of research on interoceptive awareness training — the deliberate cultivation of accurate, non-catastrophising awareness of internal bodily sensations.
Research published in Frontiers in Psychology found that individuals with better interoceptive accuracy — the ability to sense internal bodily states accurately and without distortion — show significantly lower rates of attacks and anxiety sensitivity. Consequently, mindfulness-based approaches to interoception — learning to observe internal sensations with curiosity rather than alarm — represent one of the most promising 2026 directions in treatment.
Digital CBT for Panic Attacks
Digital CBT platforms including Anxiety Coach (Mayo Clinic), Silvercloud, and Woebot have now accumulated sufficient clinical validation to be recommended alongside face-to-face CBT for attacks in many clinical guidelines. Research published in JAMA Psychiatry found digital CBT produced comparable outcomes to in-person CBT for panic disorder — with the additional advantages of immediate access, anonymity, and 24/7 availability particularly relevant for stress.
The Neuroscience of Recovery — What Changes in the Brain
Research using neuroimaging has demonstrated that successful CBT treatment of attacks produces measurable changes in amygdala reactivity — a finding with important implications. Recovery from disorder is not simply a matter of managing symptoms better. It is a genuine neurobiological change in how the brain processes threat — a rewriting of the amygdala’s threat library through repeated exposure to feared stimuli without the expected catastrophe. This provides powerful scientific grounds for confidence that recovery from attacks is not just possible but neurologically real.
Key Takeaways — Featured Snippet Optimised
Every thing you need to know about causes and symtom
- These are discrete episodes of intense fear peaking within 10 minutes — involving 4+ physical and psychological symptoms
- The neuroscience of attacks involves amygdala activation, fight-or-flight response, adrenaline and norepinephrine release
- Carbon dioxide hypersensitivity explains why hyperventilation worsens condition and why breathing control is so effective
- Clark’s Cognitive Model identifies catastrophic misinterpretation of benign bodily sensations as the primary maintaining mechanism
- Barlow’s False Alarm Theory explains why disorder develops after initial attacks
- Interoceptive conditioning explains why attacks appear to occur spontaneously
- Safety behaviours and avoidance are the primary behavioural maintaining mechanisms of stress disorder
- CBT targeting catastrophic misinterpretation and graduated exposure is the gold standard attack treatment
- Digital CBT platforms now provide clinically validated panic attack treatment with immediate access
- Understanding attacks scientifically is itself therapeutic — knowledge reduces anxiety sensitivity
A Word From Mindnesto –
At Mindnesto, we believe that understanding the science behind attacks is one of the most powerful steps toward freedom from them. Panic attacks derive enormous power from their apparent mystery, randomness, and threat of catastrophe. When you understand that is a biological false alarm — a sophisticated survival system misfiring in the absence of genuine danger — its power begins to diminish.
when you are in the state of attck it does not mean you are dying , nor does it mean you are losing control of your mind. It is a well-documented psychological response that mental healh professionals have studied extensively. Effective teatments are available.and many people ecover fully.Although the experience can feel overwhelming, it is tempoary ,manageable,and highly treatable.
Our complete practical guide on how to stop a panic attack in 5 minutes gives you the step-by-step intervention protocol. And our anxiety guide provides the daily habits that reduce the baseline anxiety from which panic attacks most commonly arise.
You are not alone in this. And you can get better. 💙
→ Read next: How to Stop a Panic Attack in 5 Minutes
→ Also read: Social Anxiety vs Shyness — The Real Difference
Frequently Asked Questions
What causes panic attacks to start?
It can be triggered by external stressors (a frightening situation, major life change, or traumatic event) or by internal physical sensations that are catastrophically misinterpreted (an elevated heart rate, slight dizziness, breathlessness from exertion or caffeine). However, according to Clark’s Cognitive Model, the fundamental cause of recurring attacks is not the trigger itself — it is the catastrophic misinterpretation of normal bodily sensations as evidence of imminent danger. This misinterpretation activates the fight-or-flight response, producing the physical symptoms that appear to confirm the catastrophe, creating a self-amplifying feedback loop.
What are the most common symptoms?
The most common symptoms — as defined by the DSM-5 — include racing or pounding heartbeat, shortness of breath, chest tightness or pain, dizziness or lightheadedness, tingling or numbness in hands and feet, sweating, nausea, trembling, feelings of unreality (derealisation or depersonalisation), and intense fear of dying or losing control. Panic attacks typically peak within 10 minutes and resolve within 20–30 minutes, although the physical and emotional aftermath can persist for hours.
Why do attacks happen at night?
Nocturnal panic attacks — waking suddenly from sleep in a state of intense fear — are explained primarily by the carbon dioxide hypersensitivity mechanism. CO₂ levels naturally rise slightly during sleep, and in people with heightened CO₂ sensitivity, this rise can trigger the amygdala’s alarm system even during non-threatening deep sleep. Nocturnal panic attacks are associated with the same maintaining mechanisms as daytime attacks — including catastrophic misinterpretation and anxiety sensitivity — and respond to the same CBT-based treatments.
How is panic disorder different from panic attacks?
A single panic attack is a discrete episode that resolves without necessarily producing lasting change in behaviour or beliefs. Panic disorder — as defined by the DSM-5 — requires recurrent unexpected attacks followed by at least one month of persistent worry about future attacks, significant behavioural change to avoid triggering situations, or functional impairment. Approximately 35% of adults experience at least one panic attack in their lifetime, but only 2.7% develop panic disorder — suggesting that it is not the initial attack but the response to it (anxiety sensitivity, avoidance, safety behaviours) that determines whether panic disorder develops.
What is the best treatment for in 2026?
Cognitive Behavioural Therapy (CBT) — specifically targeting catastrophic misinterpretation, interoceptive exposure, and the elimination of safety behaviours — remains the gold standard treatment for panic attacks, with remission rates of 70–90% in clinical trials. Interoceptive exposure — deliberately inducing feared physical sensations (by spinning, breathing through a straw, or exercising) in a safe context — is the most powerful component. Digital CBT platforms now provide clinically validated panic attack treatment with immediate access. SSRIs and SNRIs are effective pharmacological options, particularly for severe panic disorder or when CBT is not immediately accessible.
Are attacks dangerous?
No. Despite feeling extremely dangerous — including the conviction during many panic attacks that death or permanent damage is imminent — attacks are not physically dangerous. They are the activation of a biological emergency system in the absence of genuine emergency. The heart rate elevation, breathlessness, dizziness, and chest tightness produced during panic attacks are all produced by normal physiological processes and resolve completely as the alarm system deactivates. This knowledge — and the genuine experiential confirmation of it through graduated exposure — is the cornerstone of CBT
Sources and External References
- NHS — Panic Disorder
- NICE — Panic Disorder Guidelines
- NIMH — Panic Disorder
- APA — Panic Disorder
- DSM-5 — American Psychiatric Association
- Behaviour Research and Therapy — Clark Cognitive Model
- Journal of Anxiety Disorders
- Journal of Abnormal Psychology — Barlow Panic Model
- Frontiers in Psychology — Interoception Research
- JAMA Psychiatry — Digital CBT
- Mind UK — Panic Attacks
- ADAA — Panic Disorder
- NHS Talking Therapies
- NAMI — Panic Disorder
- Beyond Blue Australia — Anxiety
- CAMH Canada — Anxiety



