

By Mindnesto Editorial Team · Updated June 2026 · 11 min read
Reviewed for medical accuracy — sources cited from WHO, NHS, NICE, NIMH and peer-reviewed research on women’s mental health
Biological , hormonal,psychological,and social forces shape women’s well-being through a complex interection that creates unique patterns of vulnerabilityand resilience, yet researchers and healthcare systems have historically underserved these specific needs in the border mental health literature.If you are a woman reading this guide, your mental health experiences — the ways they manifest, the times they worsen, the social pressures that contribute to them — have a specific scientific context that you deserve to understand fully.
The data on women’s mental health is clear. 26.7% of US women experience mental illness annually, compared to 20.0% of men — meaning that more than 1 in 4 women is affected by a health condition in any given year. In the UK, nearly 1 in 4 women experiences common mental health problems in any given week. Furthermore, women are 34% more likely to experience any mental illness than men across all categories measured. Publift + 2
These figures do not represent women’s weakness. They represent the cumulative impact of hormonal complexity across the reproductive lifespan, significantly higher exposure to interpersonal trauma and gender-based adversity, disproportionate caregiving and domestic labour burdens, and a healthcare system that has historically misdiagnosed, dismissed, and undertreated women’s health concerns.
This guide gives you the complete, honest, science-backed picture of brain health — what makes it distinct, what the latest research tells us about the specific factors that affect it, and 10 evidence-based strategies designed around women’s actual lives and experiences.
We have connected this to our guides on depression mental health, burnout prevention strategies, and healthy boundaries mental health — because depression, burnout and boundary difficulties are among the most prevalent women’s health challenges in 2026.
⚠️ Medical Disclaimer: This article is for informational and educational purposes only. Women’s mental health encompasses medically complex conditions requiring professional assessment. Please consult your GP, psychiatrist, or gynaecologist about any women’s mental health concerns. Crisis support: UK — Samaritans 116 123 | USA — 988 | Canada — 1-833-456-4566 | Australia — Lifeline 13 11 14.
What Makes Women’s Mental Health Distinct — The Evidence Base
Understanding women’s mind illness requires recognising that female biology, social context, and lived experience create genuinely different patterns of mental health risk, presentation, and recovery — not simply quantitative differences from male patterns, but qualitatively different experiences that demand specific attention.
Hormones — The Lifelong Relationship
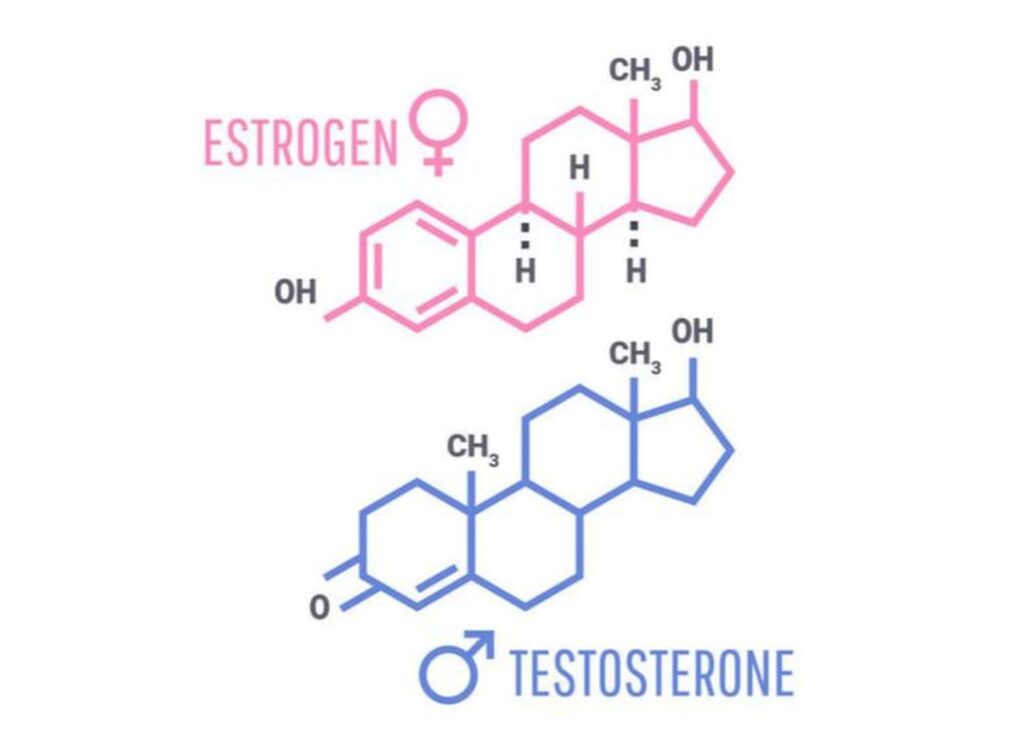
The female hormonal system directly influences women’s mental health through cyclical fluctuation in estrogen and progesterone across the reproductive lifespan, as well as through dramatic hormonal transitionduring puberty, the prenatal period,and menopause.These biological changes create measurable mental health effects that differ significantly from those experienced in male biology
Estrogen significantly influences women”s mental health through its direct interection with the serotoninsystem. By enhancing serotonin receptor sensitivity and regulating serotonin reuptake, estrogen helps maintain mood stability. Consequently ,declines in estrogen level during the prementural phase,postpartum period,and menopausal transition disrupt serotonin activity and increase susceptibility to mental health difficulties
Progesterone and its metabolite allopregnanolone interact with GABA receptors — the brain’s primary calming system — in ways that produce both anxiolytic effects at stable levels and anxiety and mood disruption during rapid progesterone withdrawal, as occurs premenstrually and postpartum.
Furthermore, the HPA axis — the stress response system governing cortisol — responds differently in female versus male biology, with women showing greater cortisol reactivity to social and interpersonal stressors specifically. This biological difference helps explain why women’s mental health is particularly sensitive to relationship quality, social rejection, and interpersonal conflict.
The Specific Women’s Hormonal Transitions
Research identifies four specific hormonal transitions as primary women’s mental health risk periods:
1. The premenstrual phase — The 7–10 days before menstruation when oestrogen and progesterone fall sharply is associated with significant women’s mental health vulnerability. Approximately 5–10% of women of reproductive age experience Premenstrual Dysphoric Disorder (PMDD) — a severe mental health condition characterised by debilitating psychological symptoms in the premenstrual phase that resolve within days of menstruation beginning.
2. The perinatal period — Pregnancy and the postpartum year represent the highest-risk women’s mental health period across the lifespan. Research published in Lancet Psychiatry found that perinatal mental health conditions affect approximately 20% of pregnant and postpartum women — yet remain significantly under-identified and undertreated.
3. Perimenopause — The 4–10 year transition preceding menopause involves dramatic oestrogen fluctuation that directly impacts women’s mental health. Perimenopausal women are 2–4 times more likely to experience a major depressive episode than premenopausal women — a women’s health risk that is frequently overlooked because the primary focus in perimenopause is on physical symptoms.
4. Menopause — The sustained low-oestrogen state of menopause produces women’s mental health consequences including increased anxiety, cognitive changes (sometimes called “brain fog”), sleep disruption, and in some women, significant mood instability — all of which deserve specific women’s mental health attention and support.
The Social and Structural Dimensions of Women’s Mental Health
Every illness is not simply a matter of biology. The social context in which women live — including disproportionate exposure to trauma, the invisible load of caregiving, economic inequality, and cultural body image pressures — creates women’s health burdens that are independent of and interactive with the biological factors described above.
The Invisible Load — A Hidden Driver
Women perform on average 2.5 times more unpaid care and domestic work than men — including childcare, eldercare, household management, emotional support for partners and children, social relationship maintenance, and what sociologists call emotional labour — the management of others’ emotional experiences and wellbeing.
This invisible load is one of the most significant and least clinically recognised mental health burdens. Research published in Journal of Women’s Health found that women who reported high levels of invisible load showed significantly elevated cortisol, poorer sleep quality, greater burnout risk, and worse mental health outcomes across all measured dimensions — even after controlling for objective workload.
Crucially, the invisible load is rarely measured in workplace wellbeing assessments, rarely discussed in clinical mental health consultations, and rarely acknowledged as a legitimate women’s mental health factor by healthcare systems. This invisibility compounds its impact.
Gender-Based Violence and Women’s Mental Health
Gender-based violence — including intimate partner violence, sexual assault, harassment, and coercive control — is one of the most significant global women’s health risk factors. Research published by the WHO found that women who have experienced intimate partner violence are twice as likely to develop depression and three times as likely to develop PTSD compared to those who have not experienced violence.
Furthermore, the cumulative traumatic stress of gender-based adversity — even at subclinical levels, including repeated experiences of discrimination, harassment, and the psychological burden of navigating gender inequality — produces measurable women’s mental health consequences through chronic HPA axis activation and amygdala hyperreactivity that closely mirror the effects of acute trauma.
Body Image and Women’s Mental Health in 2026
Body image remains one of the most pervasive women’s health challenges — and social media has intensified its impact significantly in 2026. Research published in JAMA Psychiatry found strong correlations between social media use and body image disturbance, eating disorder symptomatology, and depression specifically in women and girls.
Eating disorders — which affect women at significantly higher rates than men — are among the most medically serious women’s health conditions, with anorexia nervosa carrying the highest mortality rate of any psychiatric diagnosis. Women are nearly twice as likely as men to experience eating disorders — a women’s mental health disparity that reflects the intersection of biological vulnerability, cultural body image pressure, and trauma history.
Intersectionality and Women’s Mental Health
Mental health is not a monolithic experience. Intersecting identities — including race, ethnicity, sexuality, disability, socioeconomic status, and immigration status — create profoundly different women’s mental health experiences and access to care.
Research confirms significant women’s mental health disparities based on intersectional factors. LGBTQ+ women face significantly elevated brain health risks compared to heterosexual women — with 53.2% of lesbian, gay, or bisexual adults experiencing mental illness annually. Women of colour face compounded women’s health burdens from racial trauma and discrimination alongside gender-specific stressors — and consistently receive less adequate mental health assessment and treatment within existing healthcare systems.
10 Science-Backed Strategies
1. Track Your Hormonal Cycle as a Tool
For women of reproductive age, tracking your menstrual cycle in relation to your mood, energy, and mental health symptoms is one of the most practical and underutilised health tools available. Understanding your personal pattern of hormonal influence on mood allows you to anticipate vulnerable periods, adjust demands accordingly, and seek support proactively rather than reactively.
Digital cycle tracking apps including Clue, Flo, and Natural Cycles now incorporate mental health tracking features specifically designed for women’s health monitoring. Research published in Archives of Women’s Mental Health found that cycle-aware women’s health management significantly reduced PMDD symptom severity and improved treatment outcomes.
If you suspect PMDD or significant premenstrual mood disruption, speak with your GP — NICE guidelines now recommend both psychological (CBT, mindfulness) and pharmacological (SSRIs, combined oral contraceptive) women’s mental health interventions for PMDD specifically.
2. Seek Perinatal-Specific Support
If you are pregnant or within the first year postpartum — or supporting someone who is — perinatal women’s health deserves specific, proactive attention rather than the “is everything okay?” approach that most standard obstetric care provides.
Research consistently shows that healthcare prrofessionals identify and treat perinatalmenatl health condition earlier when they systematically screen women using validated tools such as the Edinburgh Postnatal Depression Scale (EPDS). Midwives, health visitors, and general practitioners should offer these screenings as part of routine care.
3. Understand and Address Perimenopause and Menopause as Events
The menopausal transition is one of the most significant women’s mental health events of the second half of life — and one that women are frequently least prepared for. The combination of oestrogen fluctuation, sleep disruption, identity transition, and in many cases concurrent caregiving demands creates a women’s mental health confluence that deserves comprehensive clinical attention.
In 2026,clinicians increasingly recognize menopause hormone therapy (MHT), formely known as hormone replacement therapy(HRT) , as a safe and effective first-line treatment for menopausal symstoms, including mental health challenges. Updated guidance from the British Menopause Society and growing body of evidence have strengthened support for its use. Women who experience significant nenopause-related declines in mental health should discuss MHT with their GP as part of a comprehensive mental health management strategy.
4. Address the Invisible Load as a Women’s Health Priority
Reducing the invisible load is a genuine mental health intervention — not simply a fairness issue. Research demonstrates that reducing unpaid care and domestic burden through redistribution, negotiation, or external support directly improves women’s health outcomes.
Practical invisible load strategies:
- Explicitly name and quantify your invisible load — research shows that making the invisible visible is the first step to redistributing it
- Have specific, structured conversations with partners about equitable division of domestic and emotional labour — not as a complaint, but as a women’s health conversation
- Reduce invisible load through boundary setting — our guide on healthy boundaries mental health provides a complete framework directly applicable to the invisible load
- Access domestic and caregiving support through community, family, or professional channels without guilt — reducing the invisible load is preventive health care
5. Prioritise Trauma-Informed Care
Given women’s disproportionate exposure to gender-based violence and interpersonal trauma, trauma-informed care is an essential dimension of health. Many women’s brain health presentations — including anxiety, depression, relationship difficulties, and body image concerns — have trauma roots that standard mental health assessment may miss.
Somatic approaches — body-based trauma therapies including Somatic Experiencing and Sensorimotor Psychotherapy — are gaining clinical validation for women’s mental health specifically, addressing the way trauma is held in the body rather than only in cognitive memory.
If trauma is a component of your health history, seek a therapist who specifically identifies as trauma-informed and has training in evidence-based trauma modalities.
6. Build Self-Compassion as a Core Practice
Dr. Kristin Neff’s research at the University of Texas Austin — the world’s most extensive body of work on self-compassion — consistently demonstrates that self-compassion is one of the most powerful women’s mental health protective factors available, particularly for the inner critic, perfectionism, and comparison patterns that women’s socialisation particularly promotes.
Research finds that women are more likely than men to engage in self-critical rumination — repeatedly replaying mistakes, inadequacies, and perceived failures — a pattern that significantly worsens both depression and anxiety. Self-compassion directly interrupts this pattern by replacing the critical inner voice with the kind, understanding voice you would use with a close friend.
Practical self-compassion:
- Use self-compassion breaks in difficult moments — acknowledge the pain, remind yourself that suffering is shared by others, offer yourself kindness
- Challenge the cultural norm that equates self-care with selfishness — for women specifically, the message that prioritising your own is at someone else’s expense is deeply culturally embedded and empirically wrong
- Access Dr. Neff’s free self-compassion resources at self-compassion.org
7. Protect Sleep as a Women’s Mental Health Priority Across Life Stages
Sleep and women’s health are interconnected across every stage of the female reproductive lifespan in ways that have specific implications beyond general sleep health.
Hormonal fluctuations directly affect sleep architecture in women — oestrogen and progesterone both influence sleep onset, sleep depth, and susceptibility to sleep disruption. Consequently, women report significantly higher rates of insomnia than men, particularly in the premenstrual phase, postpartum period, and menopausal transition.
Our sleep optimization guide provides a comprehensive framework for sleep improvement. Specific sleep strategies include:
- Addressing premenstrual insomnia through magnesium glycinate (400mg before bed) and consistent sleep timing
- Managing postpartum sleep disruption through sleep sharing arrangements and partner support — sleep deprivation is one of the primary women’s health risks in the first postpartum year
- Discussing sleep disruption explicitly with your GP during perimenopause — it is a legitimate mental health symptom that responds to both HRT and CBT approaches
8. Access Women-Specific Mental Health Services and Spaces
Women’s health is better served by services that understand its specific dimensions — and increasingly, such services exist in all Tier 1 countries.
Women-specific women’s mental health services:
- UK: Women’s Mental Health Taskforce resources | Mind Women’s Wellbeing | Specialist perinatal mental health teams in all NHS trusts
- USA: Office on Women’s Health — Mental Health | SAMHSA Women’s Resources
- Canada: CAMH Women’s Services | Women’s Health Clinic
- Australia: Jean Hailes for Women’s Health | PANDA
Research consistently shows that women accessing gender-specific women’s health services report higher therapeutic alliance, greater willingness to disclose trauma, and better women’s mental health outcomes than those in generic mental health settings.
9. Address Body Image as a Core Women’s Mental Health Practice
Given the significant women’s health consequences of body image disturbance — including anxiety, depression, disordered eating, and reduced quality of life — actively addressing body image is a legitimate and important women’s mental health strategy, not a vanity concern.
Evidence-based body image approaches:
- Reduce social media exposure that triggers social comparison — our digital wellness guide provides the framework for managing digital body image triggers
- Practise body neutrality rather than body positivity — research suggests that for many women, aiming for neutrality (acknowledging what your body does rather than how it looks) is more psychologically sustainable than forced positivity
- Engage in joyful movement rather than appearance-driven exercise — movement for energy, mood, and strength rather than weight management produces significantly better women’s mental health outcomes
- If body image concerns reach clinical severity — particularly if they are restricting eating, consuming significant mental space, or affecting daily functioning — please seek assessment from a therapist with eating disorder or body image expertise
10. Build YourWomen’s Support Network Intentionally
Social connection is a particularly important women’s health protective factor. Research from UCLA found that the female stress response includes a tend-and-befriend component — a distinct social-affiliative response to stress that releases oxytocin and produces genuine physiological calming — that makes female social connection particularly potent as a women’s health resource.
However, not all social connection equally supports women’s brain health. Research identifies reciprocal, genuine peer support — relationships characterised by mutual care, honest communication, and authentic connection — as the most protective social form for health, distinguishing it from social relationships characterised by social comparison, competition, or emotional labour demands.
Building your women’s mental health network:
- Invest in relationships with women who leave you feeling energised rather than drained
- Engage with women-specific support communities — including peer support groups for specific women’s mental health conditions (postpartum depression, PMDD, menopause, eating disorders)
- Be honest about your struggles with trusted women in your life — the tend-and-befriend response is activated by genuine disclosure, not by performed wellbeing
Women’s Mental Health Across the Lifespan — Quick Reference
| Life Stage | Primary Women’s Mental Health Risk | Key Protective Strategy |
|---|---|---|
| Adolescence (12–18) | Body image, social comparison, first depression onset | Media literacy, genuine peer connection, early intervention |
| Early adulthood (18–30) | Anxiety, relationship difficulties, trauma processing | Therapy access, boundary setting, secure attachment |
| Reproductive years (25–45) | PMDD, perinatal mental health, invisible load burnout | Cycle tracking, perinatal support, invisible load reduction |
| Perimenopause (45–55) | Depression, anxiety, sleep disruption, identity transition | HRT assessment, CBT, menopause-specific support |
| Menopause and beyond (55+) | Social isolation, cognitive changes, grief, purpose | Community belonging, sleep optimisation, continued therapy access |
Key Takeaways — Featured Snippet Optimised
Women’s mental health — the essential 2026 science:
- 26.7% of US women experience mental illness annually — women are 34% more likely to experience mental health conditions than men
- Women’s is shaped by hormonal complexity across the reproductive lifespan — oestrogen, progesterone, and HPA axis differences create specific vulnerability periods
- PMDD affects 5–10% of women of reproductive age. Perinatal mental health affects 20% of pregnant and postpartum women. Perimenopause increases major depression risk by 2–4 times
- The invisible load — 2.5x more unpaid care and domestic work — is a significant and clinically under-recognised women’s health burden
- Gender-based violence is one of the largest global risk factors — doubling depression risk and tripling PTSD risk
- Self-compassion, cycle tracking, perinatal-specific support, and trauma-informed care are key evidence-based women’s health strategies
- Intersectionality matters — LGBTQ+ women, women of colour, and women with disabilities face compounded health burdens requiring specific support
- Women’s mental health is best served by gender-informed, trauma-aware, hormonally literate clinical care
A Word From Mindnesto –
At Mindnesto, we believe that women’s mental health deserves a quality of information and support that actually reflects the specific complexity of women’s lived experience — not generic mental health advice with the word “women” inserted.
Your hormonal cycle is far more than a monthly occurrence-it is a sophisticated biological system that significantly influences your mental and emotional well-being. Understanding its impact is essential for maitaining overall health. The invisible load you carry every dayis not simply a matter of poor organization or time management. It is a measurable social and emotional burden that can have real psychological consequences.
Likewise, the habit of putting everyone else’sneeds before your own is not merely a personalitytrait. It is often the result of cultural expectations and conditioning that can come at the expense of your mental health. Recognizing this pattern is the first step toward creating healthier boundaries and prioritizing your own well-being
You deserve care that sees all of this. We hope this guide is a meaningful step in that direction. 💙
→ Read next: Healthy Boundaries — Why They Matter and How to Set Them
→ Also read: Burnout Prevention — 12 Science-Backed Strategies
Frequently Asked Questions
Why do women have higher rates of mental health conditions than men?
Its reflect multiple intersecting factors. Biologically, hormonal complexity across the reproductive lifespan — including cyclical oestrogen and progesterone fluctuations — creates specific vulnerability periods with no male equivalent. Socially, women face disproportionate exposure to interpersonal trauma, gender-based violence, and invisible care labour burdens that directly impact women’s
What is PMDD and how does it affect ?
The menopausal transition produces mental health effects through multiple mechanisms — primarily through the impact of declining oestrogen on the serotonin system and sleep architecture. Perimenopausal women are 2–4 times more likely to experience a major depressive episode than premenopausal women.
What is postpartum depression and how common is it?
Postpartum depression (PPD) is a clinical women’s mental health condition affecting approximately 10–15% of new mothers — characterised by persistent low mood, anxiety, difficulty bonding with the baby, exhaustion beyond normal new-parent tiredness, and in severe cases, thoughts of self-harm. PPD is distinct from the “baby blues” — which affect up to 80% of new mothers in the first two weeks and typically resolve spontaneously. PPD requires professional women’s mental health treatment. In the UK, PANDA UK and NHS Perinatal Mental Health Teams provide specialist support. In the USA, Postpartum Support International offers helpline support on 1-800-944-4773.
How does trauma affect women’s mental health specifically?
Trauma affects women’s mental health in specific and significant ways. Women are more likely than men to experience interpersonal trauma — including intimate partner violence, sexual assault, and childhood abuse — and to develop PTSD following traumatic events, with research suggesting that women are twice as likely to develop PTSD after trauma exposure as men with comparable trauma histories.
Where can women get specific mental health support?
UK: Mind UK | NHS Talking Therapies | Pandas Foundation | Samaritans — 116 123
USA: SAMHSA Women’s Resources | Office on Women’s Health | Postpartum Support International | 988 Lifeline
Canada: CAMH Women’s Services | Women’s Health Clinic
Australia: Jean Hailes for Women’s Health | PANDA — 1300 726 306 | Beyond Blue
Sources and External References
- WHO — Gender and Women’s Mental Health
- NHS — Women and Mental Health
- NICE — Perinatal Mental Health
- NICE — Menopause Guidelines
- NIMH — Women and Mental Health
- SAMHSA — Women’s Mental Health
- Journal of Women’s Health
- Archives of Women’s Mental Health
- Lancet Psychiatry — Perinatal Mental Health
- JAMA Psychiatry — Social Media and Body Image
- Mental Health Foundation — Women Statistics
- Self-Compassion.org — Dr Kristin Neff
- Postpartum Support International
- PANDA Australia
- Jean Hailes for Women’s Health
- Pandas Foundation UK
- Mind UK
- CAMH Canada
- Beyond Blue Australia
- Office on Women’s Health USA